
We hope our latest edition of Health Matters – on the subject of “Preventing ill health from alcohol and tobacco”– will help you and other health professionals by compiling key facts, figures and evidence of effective interventions. This professional resource makes the case for why NHS providers should implement the ‘preventing ill health by risky behaviours – alcohol and tobacco CQUIN’.
Where we can, we’re also committed to answering your questions and taking on your feedback. In this blog we’ve published the answers to a number of Health Matters questions we received from professionals across the UK at the recent launch teleconference.
Question 1 (Hospital based training on very brief advice on smoking (VBA) for smoking cessation)
My question is around the VBA training for smoking cessation. The one that's available on the National Centre for Smoking Cessation & Training (NCSCT) website is excellent, but geared towards primary care. Are there plans to produce a more ward-based or hospital-based video and training?
Answer
Thank you for being complimentary about the NCSCT VBA training for smoking cessation. PHE aims to be responsive to what people need and will find helpful. Recently we've developed specific modules for midwifery. We will take your comment on board about developing hospital-tailored training as well.
Question 2 (Funding for smoking cessation services)
How is Public Health England supporting public health departments in councils either to ring-fence funding or to make it a high priority so that funding is applied to smoking cessation services locally?
Answer
The public health grant is ring-fenced for public health but not for any particular topic within public health. PHE is interested in maximizing the impact of the CQUIN and the provision of evidence-based quitting support for smokers is central to that, whether that support is provided on site or in the community.
PHE is supporting the local system, including funding decisions, by:
- publishing data on local need alongside commissioning support packs that will help Health and Wellbeing Boards to plan for needs in their local area
- developing tools – for example CleaR for both tobacco and alcohol - that will help make sure that local partnerships share a vision and focus on how they want to celebrate and improve
- continuing to support the local system through our work at centre levels
Furthermore, in our supplementary guidance to the CQUIN, we strongly advised collaborative working across the health and care system, including local government. It will be critical that discussions between local partners start early and that the agreed pathways for patients are as smooth as possible. Local system level partners need to agree on a local solution, and areas will differ in terms the type and level of support that is provided.
The main requisite is that there is agreement between providers and the local public health department on referral pathways to quitting support. It's critical that providers join up with colleagues in the local authority to establish what is going to be available for patients when they need to follow a pathway into a local service. If you are having trouble with that, do come back to us because we are happy to help by supporting that engagement and conversations at the local level.
Question 3 (Mismatch between cut to public health grant and the need for additional services)
I'm a public health specialist and I've been doing lots of work on trying to bring forward a hospital stop smoking service. The key issue that we have is the post-discharge support. Obviously, most patients aren't in hospital very long and the difficulty we have locally, and I'm sure it's reflected from colleagues around the country is that the cut back to the public health grant to local authorities means that many stop smoking services have been cut back, in some cases completely. Now we have this CQUIN, which potentially delivers very large numbers of smokers into those services, which simply will not have the capacity to cope with the numbers that are coming through.
Locally, we've been working very closely with the NHS, with our trust, with our CCG and we've put forward a business case, which has been well received by clinicians but it hasn't got funding. One of the key things is that for many people who are discharged, they wouldn't necessarily be physically able to attend say a stop smoking group in the community. So we were looking particularly at post-discharge telephone support using the Ottawa model that's been so successful over in Canada. But that does require additional resource and I think the fundamental issue that we have here is that obviously the NHS trusts are being incentivised to a degree to adopt the CQUIN and take the measures internally and then refer onwards.
Nationally we seem to have a mismatch with the public health grant to local authorities being cut at the same time as NHS England is seeking to push a lot more business towards those local authority services, which may not have the capacity. Is this being addressed at the national level?
Answer
We are acutely aware that providers that are implementing the Preventing ill health CQUIN will want to assure themselves that patients receive the right interventions and treatments. One of the things that needs to be in place to make this work is for there to be agreement at a local level about how referrals to specialist stop smoking support can be implemented. It may be that evidence-based support can be made available in settings other than just a local stop smoking service as we've known them. For example, different approaches include jointly commissioned services, sometimes hospital based, and minimum provision of pharmacotherapy and behavioural support provided by a trained member of staff. One Region is also trialling phone based smoking cessation support.
It is critical that the NHS and local authorities join up to ensure that there is appropriate support for people to enable this CQUIN to really fly. So you have identified something that's close to our hearts and something that is critical to the success of the Preventing Ill Health CQUIN.
Question 4 (Achieving the CQUIN and contract payments)
Is there an expectation then when we put this into contracts that there will be an additional cost for those contracts?
Answer
The 2017/2019 CQUIN scheme applies to commissioners and providers using the NHS Standard Contract. The Scheme is worth a maximum of 2.5% that is payable in addition to the Actual Annual Value, depending on provider performance.
The Preventing ill health CQUIN is worth a minimum weighting of 0.25% and is applicable to Mental Health and Community providers between 2017 to 2019 and Acute providers in 2018/2019. To achieve full payment for the Preventing ill health CQUIN, providers must meet three milestones in quarter one and then meet set thresholds from quarter two and onwards.
The advice remains the same for Block Contracts, Accountable Care Service Agreements, and Capped Spend Contracts. The CQUIN Guidance for 2017-2019 provides more information about eligibility and payments. For a specific query about how a contract should interact with the CQUIN, please send details to e.cquin@nhs.net.
Question 5 (Benefits of the CQUIN to providers)
Many providers are now on block contracts and it's unclear how the CQUINs interact with that. The value of this CQUIN is relatively low compared to the other CQUIN targets that are coming out and it's sometimes difficult to get boards to pay attention to this compared to setting up other services, especially when an acute trust is looking at training up all members of staff to provide very brief advice; it's quite a big undertaking and a large piece of work for us but the tariffs don’t seem to really reflect that especially given the importance of smoking cessation.
Answer
The CQUIN Guidance for 2017-2019 confirms that “any provider of healthcare services commissioned under an NHS Standard Contract is eligible for CQUIN. This is inclusive of the independent sector. NHS England has advised PHE that this advice remains the same for Block Contracts, Accountable Care Service Agreements, and Capped Spend Contracts. For a specific query about how a contract should interact with the CQUIN, please send details to e.cquin@nhs.net.
In terms of the tariff values, we appreciate that there's a lot of work involved for the tariff that's being offered. To engage Boards, in addition the minimum of 0.25% of the value of the annual contract, it’s useful to focus on the longer term outcomes that are achievable from commitment to delivering IBA and VBA well. Now, that's not always reflected in the end of year contracting round, but if we do deliver the CQUIN as best as we can and achieve the clinical standards that we would like to, then we will get better clinical outcomes and cost savings.
It is estimated that the successful implementation of the Preventing Ill Health CQUIN can lead to net savings to the NHS of:
- £13 per patient referred to stop smoking support and prescribed Nicotine Replacement Therapy each year over five years
- £27 per patient receiving alcohol brief advice each year over five years, from reduced alcohol-related hospital admissions following improvements in morbidity
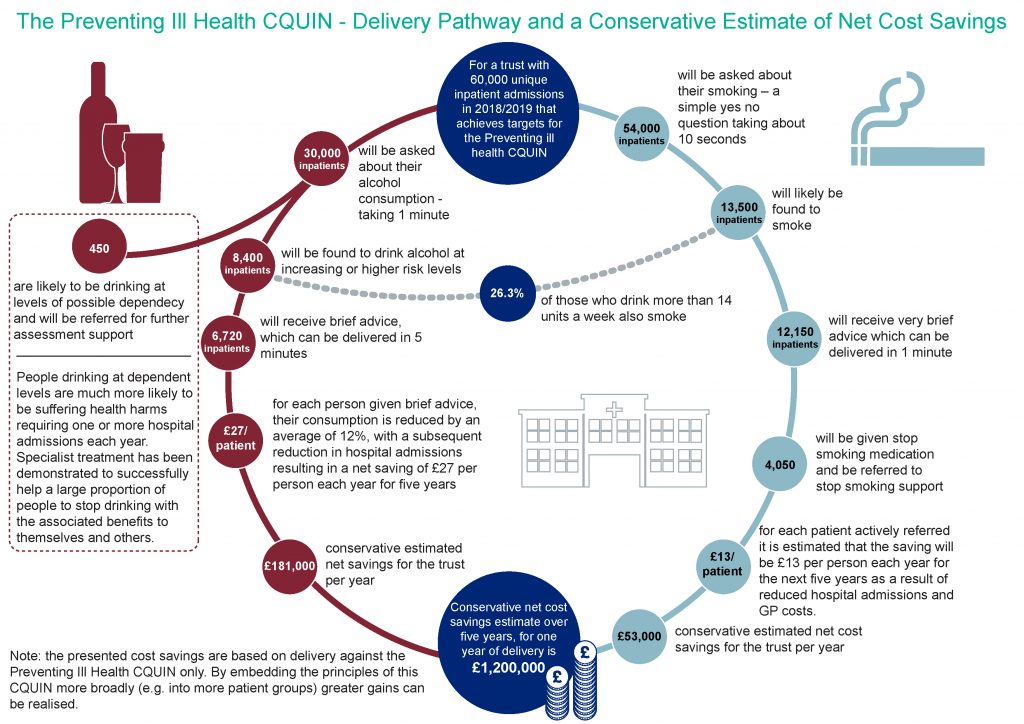
Public Health England’s Public Health Data Science Team has developed this infographic to show the CQUIN delivery pathway and estimated net cost savings. Download this and the full set of Health Matters infographics for this edition.
Engaging leaders and having visible leadership within a hospital trust is very important to the success of the CQUIN. In the latest Health Matters, PHE called on providers to facilitate successful delivery of the preventing ill health CQUIN by ensuring that there is strong leadership at all levels of the trust and that staff members feel supported to deliver these interventions as part of usual care.
Question 6 (Training for CQUIN 3 as well as CQUIN 9)
I work for a Mental Health Trust and I'm responsible for leading on both CQUIN 9 and CQUIN 3, both of which impact on mental health and physical healthcare and are very linked for our service users. I was just wondering on this sort of training package side of things, whether there are any opportunities or plans for creating a training package that covers our requirements for CQUIN 3 as well as for CQUIN 9. CQUIN 3 is around cardio-metabolic assessments for all people in our mental health services, both community and in-patients and obviously includes alcohol and smoking assessments and brief advice. There are time pressures and in terms of efficiencies and effectiveness across NHS providers, it would be really useful to have something created centrally that we could all use.
Answer
That's a very good point, the Preventing ill health CQUIN (CQUIN 9) and the Physical healthcare for people with serious mental illness (CQUIN 3) do complement each other. We haven't looked into developing training module that would cover both modules, but we can consider whether this is feasible and appropriate as we look forward to providing ongoing support to providers implementing both of these CQUINs.
Question 7 (Learning development to support a smoke free NHS)
We're from an acute trust in London and we work in a learning development department which is a centralised corporate function. What role would you see a function such as ours having in relation to this? We deliver staff training, predominantly on soft skills, personal development etc.
Answer
There's a key role for you in terms of looking at training plans, and we know that some providers have started to mandate training around doing brief interventions for alcohol and tobacco. But we also understand that there are opportunities to learn from some of the training that has been imparted, and to learn from the sort of interactions that staff are having. We’re now looking a bit more around what we can learn from behavioural insights and checking whether we are having the impact that we're trying to achieve. What we’re learning, is that it's not only about setting up the baseline training to make sure that people can have confidence in delivering these interventions. It’s also looking then at whether they are being delivered in the best and most optimised way in order to get the best outcomes that we can.
With the aim to go smoke free in the NHS, one of the big issues we've got at the moment, responding to feedback from commissioners in particular, is the cultural shift required. There’s work to be done in supporting clinicians to start treating tobacco dependency. What is it that we can do with frontline staff, as they are the important advocates of this? There is the potential for some real cultural shifts here as well. Organisations are looking not only at induction but throughout the whole training and development of staff in local hospitals. It's not only induction but it's also looking to annual training, refresher training, and also targeting particular project and audit work, for example, and quality improvement work across all members of staff.
Question 8 (The CQUIN requirement for referral and the offer of stop smoking medication)
I work in an acute trust and I noticed that the numerator for indicator 9C is about eligible patients being referred and offered stop smoking medication. My clinical experience is that quite often when people are initially admitted to hospital they might not be particularly receptive to stopping smoking, it can feel like a really big thing. But we would prescribe nicotine replacement therapy (NRT) to help with withdrawal and then, perhaps later, they might be more receptive because they have gained that personal confidence that they've gone without smoking because we're a smoke free site. Our data system will collect that initial assessment, which may well be a decline on offered referral to the stop smoking service. We will prescribe NRT but that wouldn't be seen as a positive outcome on the CQUIN - I think it does have to be referral and medication, not just one or the other to be compliant with Indicator 9C – does the panel have any thoughts or comments on that?
Answer
It’s great to hear that you are following up with patients who initially turn down further support to stop smoking, to ensure that if these patients feel more prepared to quit at a later date then they are given support to do so.
You're correct that the indicator 9c requires both an active referral for further support to be made and the offer of stop smoking medication. Both of these actions need to be met in order to achieve 9c. This requirement is based on the evidence that people are more likely to quit if they are supported with pharmacotherapy and behavioural support. The 30% target is consistent with evidence that of those who are offered a referral, 30% are likely to accept this offer.
To accurately reflect your current good practice and to allow you to capture this information for CQUIN purposes, it would be ideal if your information systems could be updated to capture this information. If you are using electronic patient records, it’s likely that this small change could be logged as a ‘change request’. It’s advisable to undertake a systems audit as early as possible to allow time for all needed changes to be made to your information systems prior to the beginning of the CQUIN.
Question 9 (How has the CQUIN fared where it has already been implemented)
I understand that the CQUIN has been running in mental health community settings over the last six months or so. I know it's early days but I'd be interested to see if there's any response on how that's going and if there's any good practice that we can pick up on. Most of the questions have been around smoking cessation so far. I'm interested that the alcohol part of the CQUIN is particularly focused on risky behaviours, that is those people scoring probably above six on the audit score, who are not necessarily alcohol dependent. This strikes me as a very high emphasis on the Identification and Brief Advice (IBA) bit, which is going to be quite a challenge, I think. So your advice on that is welcome.
Answer
You're absolutely correct that the intent here is to find people who aren't alcohol dependent and that the real push here is to deliver IBA in these settings. You are also right that there is a challenge in getting this up to scale, which is where your learning and development people, creating the time to support staff to get the skills to be able to do this, is going to be critical. We have provided some relatively brief IBA training, which is hospital specific through the E-learning for Health portal (This can also be accessed through ESR). This training will help in terms of getting people skilled up. Alcohol Care Teams in hospitals will also be a useful resource in terms of providing peer-to-peer support and helping staff in different roles across the organisation to take this on.
You asked about best practice and we have published a case study from the South London and Maudsley NHS Foundation Trust which is very much focused on what they've done to embed and deliver alcohol IBA for this CQUIN. They’ve implemented some great changes and it provides a really excellent study of how a Mental Health provider has taken on this CQUIN.
Summary
If you have any further questions, the alcohol and tobacco teams here at Public Health England will be pleased to answer them. So please send your question by email to healthmatters@phe.gov.uk. For technical queries about the CQUIN, please email the dedicated CQUIN team at e.cquin@nhs.net.
Do please keep on sharing your stories about how you have used the Health Matters materials to communicate your messages and to get things done, or if you have ideas for improvements. Just send an email to healthmatters@phe.gov.uk.
Health Matters
Health Matters is a resource for professionals which brings together the latest data and evidence, makes the case for effective public health interventions and highlights tools and resources that can facilitate local or national action. Visit the Health Matters area of GOV.UK or sign up to receive the latest updates through our e-bulletin. If you found this blog helpful, please view other Health Matters blogs.
1 comment
Comment by Mr R W Ebley posted on
Site didn't say comment awaiting moderation when I just posted this
In order that change is effectively undertaken all levels of government and other public funded organisations need to demonstrate good management
I suggest independent management accreditation (eg ISO 9001) to achieve this
Thank you
Mr R W Ebley