
 We are very fortunate in England to have some of the best primary care services in the world. We also have amongst the most computerised general practices, and primary care activity and clinical information is recorded in real time at the point of consultation. Over 95% of the population see their GP at least once every two years and there are more than 300 million consultations a year. The data collected in primary care is rich, complex and vast.
We are very fortunate in England to have some of the best primary care services in the world. We also have amongst the most computerised general practices, and primary care activity and clinical information is recorded in real time at the point of consultation. Over 95% of the population see their GP at least once every two years and there are more than 300 million consultations a year. The data collected in primary care is rich, complex and vast.
From a population health perspective, being able to use and analyse the data collected in primary care has transformational potential. The quality and outcomes framework has been a major step forward – there is evidence that it has had tangible, if modest benefits on health outcomes, and it has produced information which would be otherwise be difficult to collect at any scale. We now have registers of a wide range of chronic diseases and estimates of disease prevalence, intermediate outcome measures (e.g. diabetes and blood pressure control) and highly disaggregated data on some aspects of lifestyle (GP-recorded obesity, offers of lifestyle intervention in hypertension and so on).
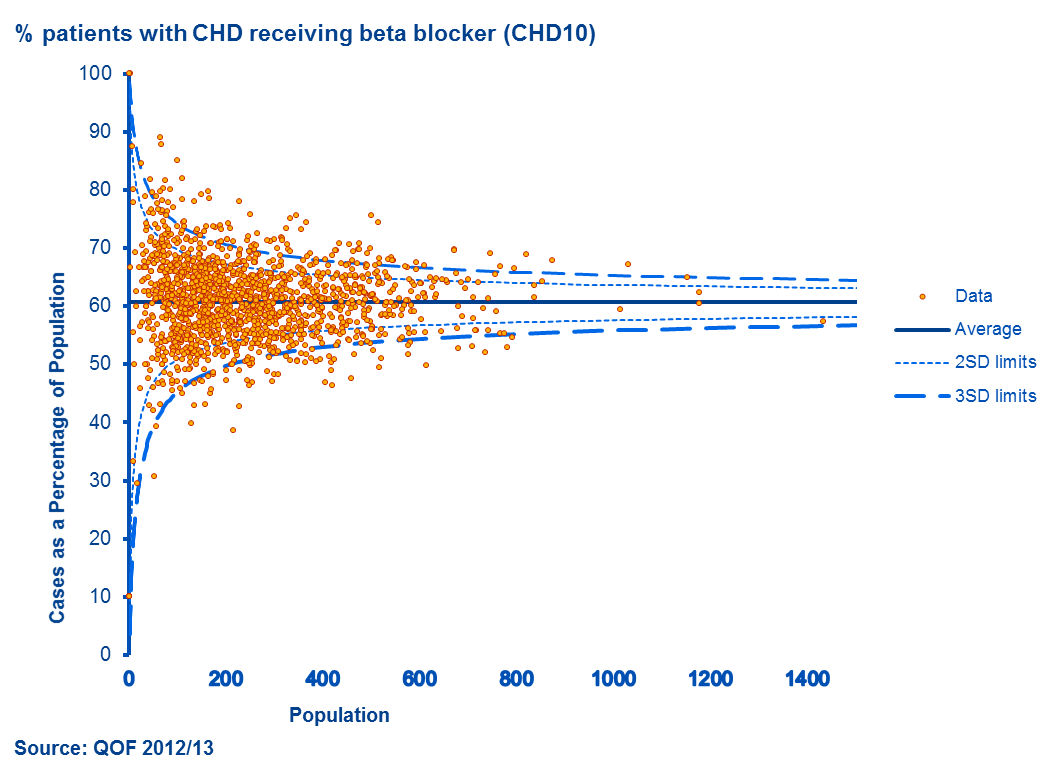
Source: QOF 2012/13

Source: QOF 2012/13
We have a much better understanding of the variation in quality of care in general practice and tools like practice profiles to help us. These show, for example, that there is considerable variation between practices in the prescribing of beta blockers for secondary prevention of coronary heart disease. In treating CHD using beta blockers to reduce mortality is cost effective (one study estimates a cost of 200 pounds per life year gained). On average 60% of CHD patients receive a beta blocker, but in about 10% of practices rates are significantly higher this. There may be many good reasons why practices don’t achieve higher rates of prescribing, but imagine if we could shift the average rate of beta-blocker use to 70%? Around 3,000 practices would need to increase their prescribing to have rates consistent with the new average, with 50,000 more people being treated, and potentially 1000 life years saved per year at relatively low cost.
Primary care data can tell us lots more. For instance, how many people smoke; levels of obesity; who is referred for exercise programmes, and much about local health inequality. It can give population estimates of the distribution of blood pressure and help us evaluate interventions to shift that distribution, helping to reduce prevalence of hypertension and reduce stroke. It can be triangulated or combined with data from surveys and other sources. The potential is endless.
Of course data on its own doesn’t save lives, but appropriate analysis of good quality data can support action that will. However, Chris Carrigan noted of some of the issues in using big data in his blog a few days ago in relation to the scope and scale of cancer data and its power to transform care for people with cancer. He pointed out some of the recent media furore there has been about “big data” and large scale national databases, and the need to engage with patients in the use of their data. So it is with primary care data and the “pause” in the roll out of Care.data.
We in Public Health England need to play our part in engaging with the public and the professions to join us on this exciting journey, to understand why access to primary care information is important and its potential to transform the quality of care each of us receives. Once trust has been damaged, winning it back is a tough task and that is the situation this project faces now. The conversation with the public has started and needs to be continued.
At the same time that Care.data was headline news two Danish public health students were visiting our Knowledge and Intelligence Team to learn about what we do and about the contribution of health intelligence to improving public health in the England. The Danish students were surprised at how far behind England is to what they are used to in Denmark where sharing primary care data is normal not controversial; crucial, not risky. This is where we need to get to in England, and quickly.
Featured image via NHS Image Library. Used under Crown Copyright.
2 comments
Comment by Bren posted on
Hello Julian and Claire,
Thank you for a really good and informative read on this area of continued discussion .
One of the points I took from your blog was the huge opportunity to connect, to gather to gain data and information form a huge part of the people and communities in England. The other aspect was around trust on, both ascertaining and using the data. My only other thought would be, and care.data is no exception, is it is beyond seeking and gaining trust, it is absolutely maintaining the trust. We have to earn trust too. .
I think the rich source of data is crucial for going forward in primary care, and integrating care as a whole, and one area I would welcome it being used is in tacking inequalities in areas such as diagnosis, treatment and after care. This being in terms of both information and access to services for seldom heard, undeserved, and vulnerable people and communities. I also think it could be used to support people in transition both within and between services.
Thank you for the well presented blog,
Best wishes,
Bren.
Comment by Brian Reed posted on
Dear Sirs, Your conclusion that we are fortunate in England to have some of the best primary care services in the world does not tell the whole story. While I would agree that on the whole we may have 'some' of the best care but not every aspect bears scrutiny. There are areas where access to primary care is considerably restricted by very long waiting times for appointments, for example.